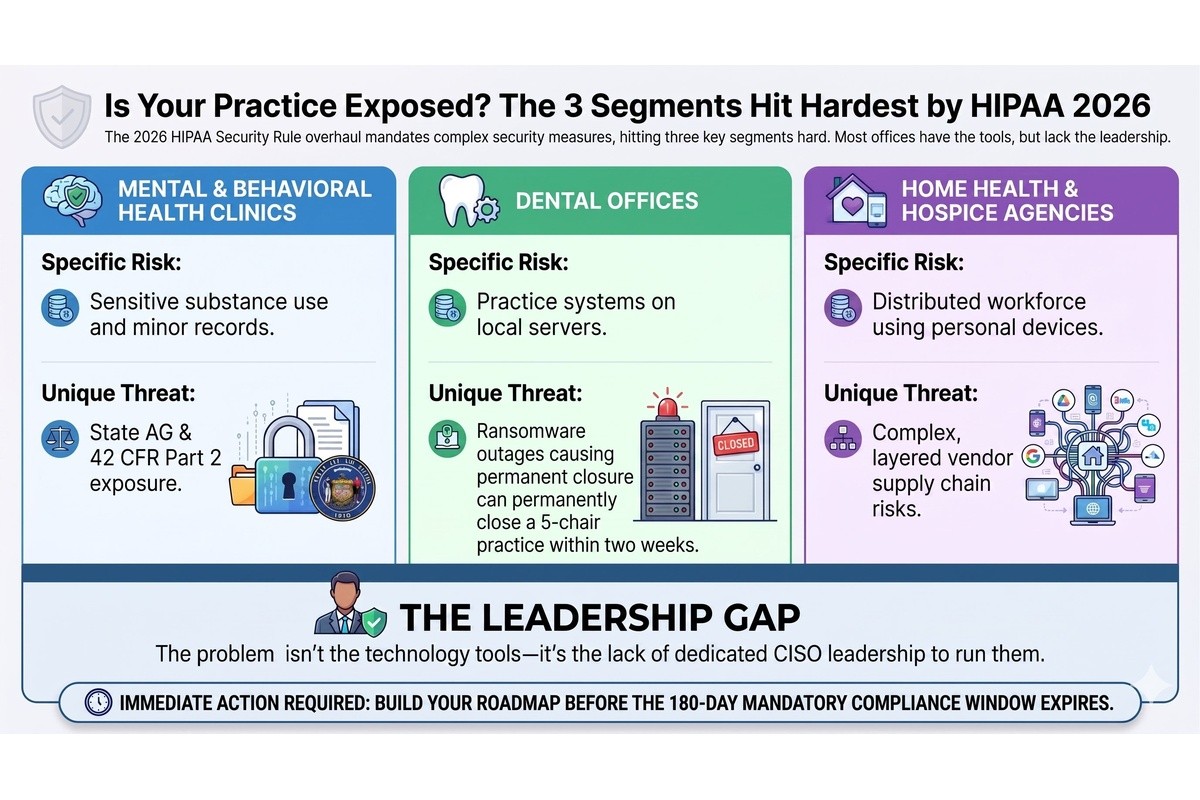


If you are the Executive Director or Administrator of a home health or hospice agency, you are likely managing one of the most complex, distributed workforces in the healthcare industry. Your clinicians are constantly on the move, delivering critical care in living rooms, assisted living facilities, and everywhere in between. You are balancing patient schedules, billing complexities, and the constant pressure of maintaining high-quality care. But beneath the surface of this operational balancing act lies a growing, often ignored risk: the cybersecurity of your remote workforce.
The reality is that home health and hospice agencies operate outside the traditional, secure perimeter of a hospital or clinic. Your "office" is wherever your nurses and therapists happen to be. This distributed model creates a massive security surface area that most agencies simply have no plan to manage. And while you might assume your IT provider has this covered, the truth is that keeping the servers running is very different from protecting patient data across dozens of unsecured locations.
In a traditional clinical setting, IT teams can build a fortress around the network. They control the firewalls, the Wi-Fi access points, and the devices connected to them. In home health, that fortress does not exist. Your perimeter is defined by the devices your staff carry and the networks they connect to throughout the day.
This creates a unique set of vulnerabilities. When a nurse accesses an Electronic Health Record (EHR) from a patient's home, they are operating outside your direct control. If that device is compromised, or if the connection is intercepted, the sensitive Protected Health Information (PHI) they are accessing is suddenly at risk. The challenge is not just technical; it is operational. How do you enforce security policies when your staff rarely step foot in the main office? How do you ensure that the convenience of remote access does not become the downfall of your agency's compliance?
Many home health agencies rely on a Bring Your Own Device (BYOD) model to save costs and provide flexibility. Clinicians use their personal smartphones or tablets to check schedules, communicate with the office, and even access patient records. While this seems efficient, it introduces significant risks to home health PHI security.
When a clinician uses a personal device, that device is often shared with family members, connected to public Wi-Fi networks, and loaded with personal apps that may not be secure. If a nurse's child downloads a malicious game on the same tablet used to access your EHR, your agency's data could be exposed. Furthermore, if a personal device is lost or stolen, do you have the ability to remotely wipe the agency's data without wiping the clinician's personal photos and contacts? Without a formal BYOD healthcare policy and Mobile Device Management (MDM) software, you are essentially trusting the security of your patient data to the personal habits of your staff.
The risks extend beyond the devices themselves to the networks they connect to. When your staff work from home—whether it is a clinician finishing notes at the end of the day or an administrative team member handling billing—they are likely using their personal home Wi-Fi networks.
Home Wi-Fi networks are notoriously insecure. They often use default passwords, outdated encryption protocols, and are shared with numerous smart devices, from televisions to refrigerators, any of which could be compromised. If a hacker gains access to a staff member's home network, they can potentially intercept the data being transmitted between the clinician's laptop and your agency's servers. This is a critical vulnerability in remote workforce HIPAA compliance. Without secure connections, such as Virtual Private Networks (VPNs), every home office becomes a potential entry point for a breach.
Your agency relies on a web of third-party vendors to operate: billing software, telehealth platforms, scheduling applications, and secure messaging tools. Under HIPAA, any vendor that creates, receives, maintains, or transmits PHI on your behalf must sign a Business Associate Agreement (BAA).
However, simply having a signed BAA filed away is not enough. BAA failures occur when agencies assume that a signed document equates to actual security. Are you verifying that your billing vendor is actually encrypting data at rest? Do you know if your telehealth platform has experienced a recent breach? If a vendor experiences a security incident and exposes your patients' data, your agency is still ultimately responsible. Managing vendor risk is a continuous process, not a one-time paperwork exercise. Failing to actively monitor your vendors is a significant gap in home health agency HIPAA compliance.
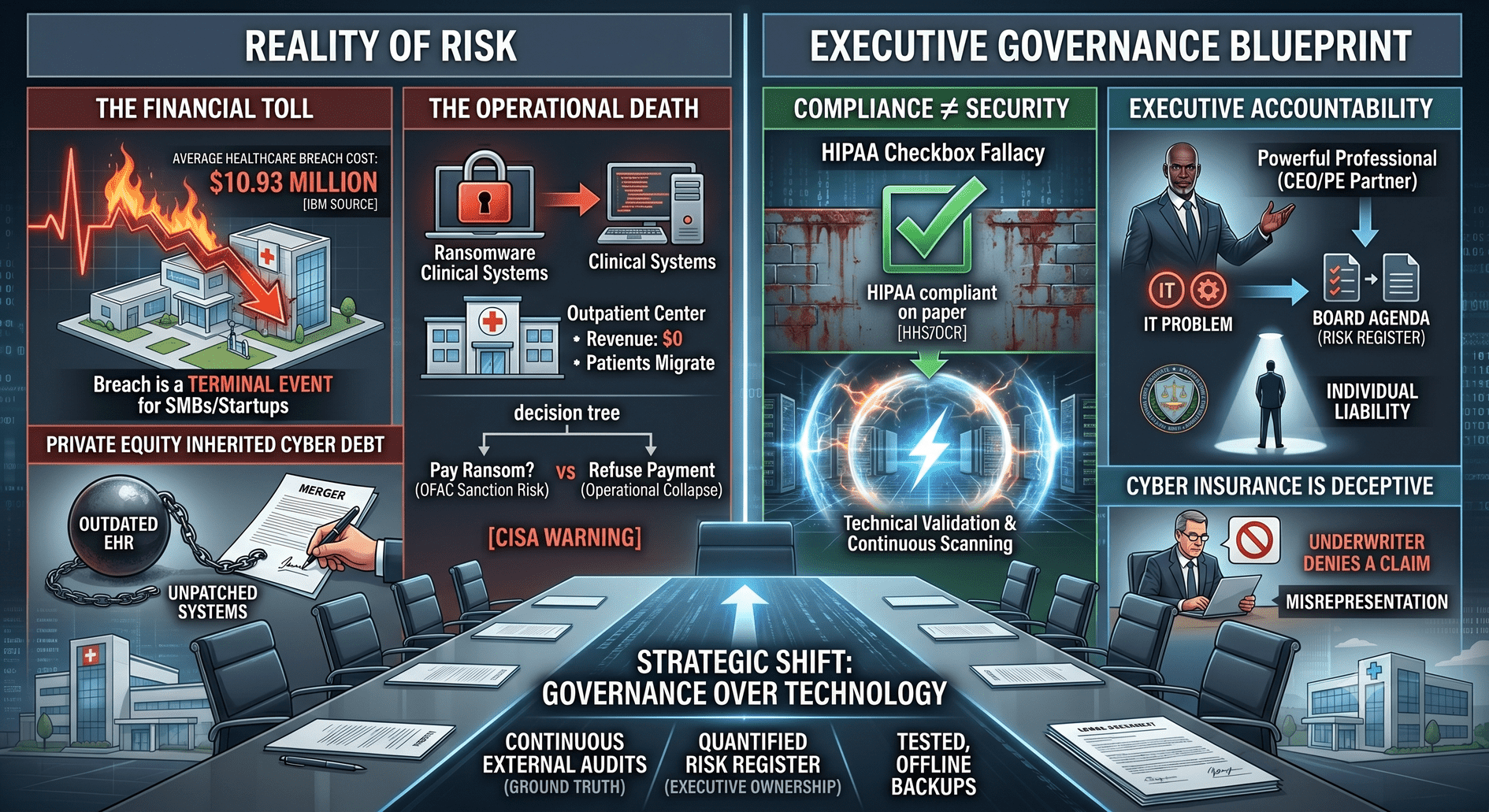
The consequences of these unmanaged risks often become painfully clear during a state audit or a Joint Commission review. Auditors are increasingly focusing on the technical safeguards required by the HIPAA Security Rule, particularly for agencies with distributed workforces.
Imagine an auditor asking for your risk analysis regarding remote access, or requesting proof that all mobile devices accessing PHI are encrypted. If your answer is that you rely on your staff to be careful, or that you assume your IT guy handles it, you will likely face significant findings. These gaps can lead to corrective action plans, fines, and a loss of trust from the hospitals and health systems that refer patients to your agency. A failed audit is not just a compliance issue; it is a business risk that can impact your revenue and reputation.
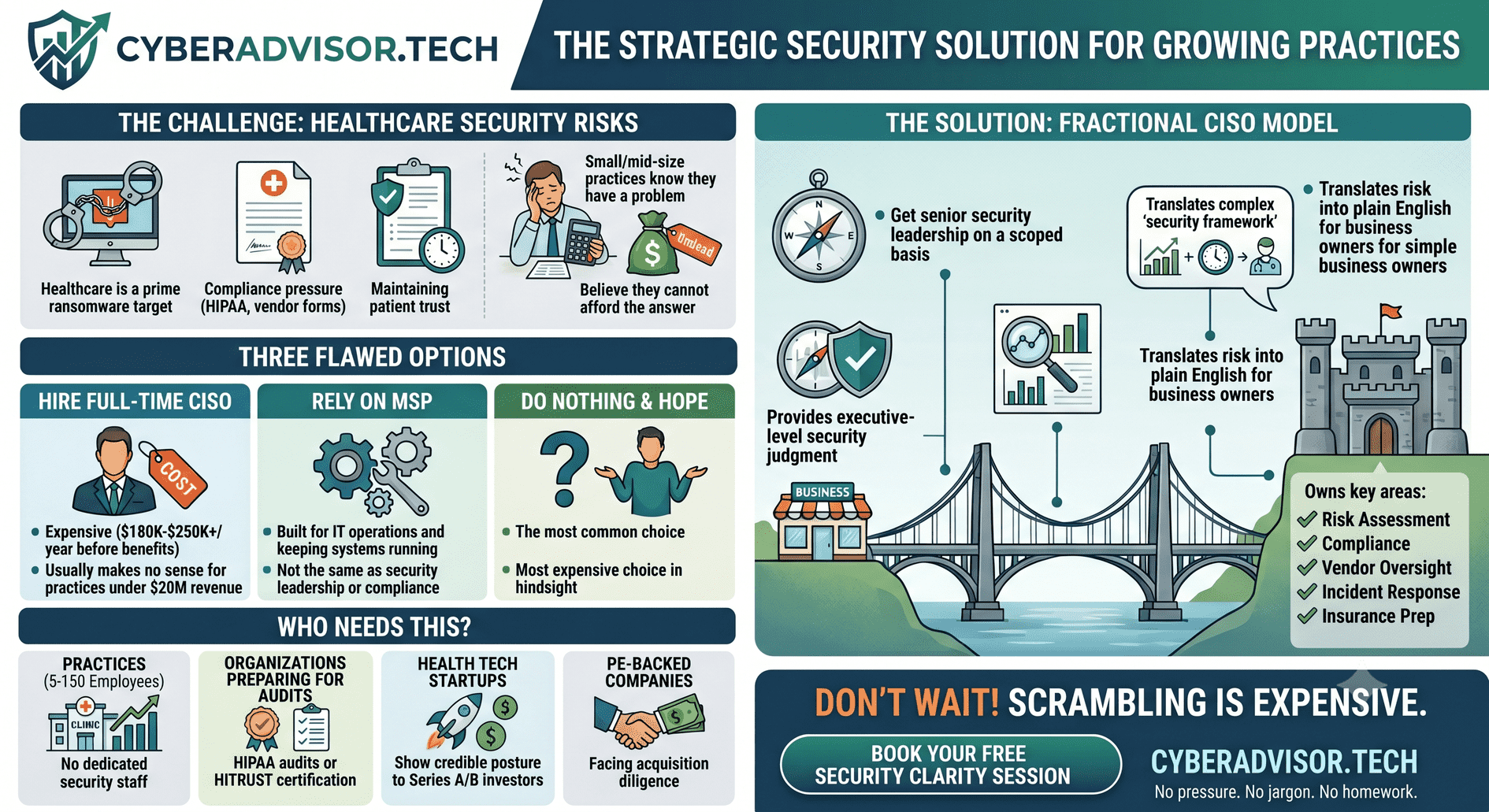
This brings us to a critical distinction: the difference between having IT support and having a security strategy. Your Managed Service Provider (MSP) or local IT guy is essential for keeping your systems running, resetting passwords, and fixing broken laptops. They are focused on operations and uptime.
Cybersecurity, however, is about governance, risk management, and compliance. It requires someone who understands the specific regulatory requirements of hospice cybersecurity and can translate those requirements into actionable policies. An IT provider might install antivirus software, but a security leader will ensure that your BYOD policy aligns with HIPAA requirements, that your vendor BAAs are actively managed, and that your staff are trained to recognize phishing attempts. You need both functions, but assuming your IT provider is handling your strategic security is a dangerous misconception.
Addressing these risks can feel overwhelming, especially when you are already stretched thin managing the day-to-day operations of your agency. However, you do not need a massive budget or a full-time Chief Information Security Officer (CISO) to start making meaningful improvements. Here are practical first steps you can take:
You don't need a full-time CISO. But you do need someone who thinks like one. As a former CEO, I understand the operational pressures you face. I know that security initiatives must align with your business goals, not hinder your clinicians' ability to provide care.
If you are unsure where your agency stands, or if you are concerned about the security of your distributed workforce, let's talk. I offer a free, 30-minute Security Clarity Session. We will discuss your specific challenges, without the jargon, and you will leave with a clearer understanding of your security posture—whether we work together or not.
Book Your Free Security Clarity Session Today and take the first step toward protecting your patients, your agency, and your peace of mind.
Connect with Melissa Thornton on LinkedIn